Functional Risk Part 1 – What Causes It?
I like to think that I have three things I provide to my dental patients:
- Risk assessment – helping them understand and fully own risk factors for their long-term dental health
- Risk management – helping them understand what they could do to manage that risk
- Damage repair – definitively treating a risk that was not completely managed
Many dentists do not pay attention to occlusion unless it is a problem for the patient or unless it becomes an issue in treating the patient. As I tell dentists in Essentials 1: Aesthetic& Functional Treatment Planning, assessing functional risk is as important to me as assessing other risks, such as caries or periodontal disease. I want to find the signs of functional risk, so if a patient has higher risk of damaging teeth from excessive loading, I can help the patient understand that risk and the options for managing it.
Functional Risk Assessment
In a previous blog, Occlusal Wear Part 1: Is it advancing? How fast?, I shared the mental game I play with every patient and the ways in which I document wear changes. With every patient, I ask myself, “Is the wear I see on the teeth normal for the patient’s age? Is it advancing at a pathological rate?”
I categorize patients in one of three functional risk categories:
- Mild
- Moderate
- High
The patients I place in the high-risk category are those whose functional wear and tear is more than it should be for their age. Their teeth are breaking down noticeably faster than the average rate.
In my practice, we measure from the CEJ to the incisal edge of several teeth with wear. We take the measurement on the mid-facial and record it on the patient’s perio chart. At subsequent appointments, we can now repeat these measurements and have clear data showing that the process is continuing. Other great ways to document tooth wear are with photography and digital impressions. We compare scans months later and get a precise measurement of the change.
What causes someone to be at higher functional risk?
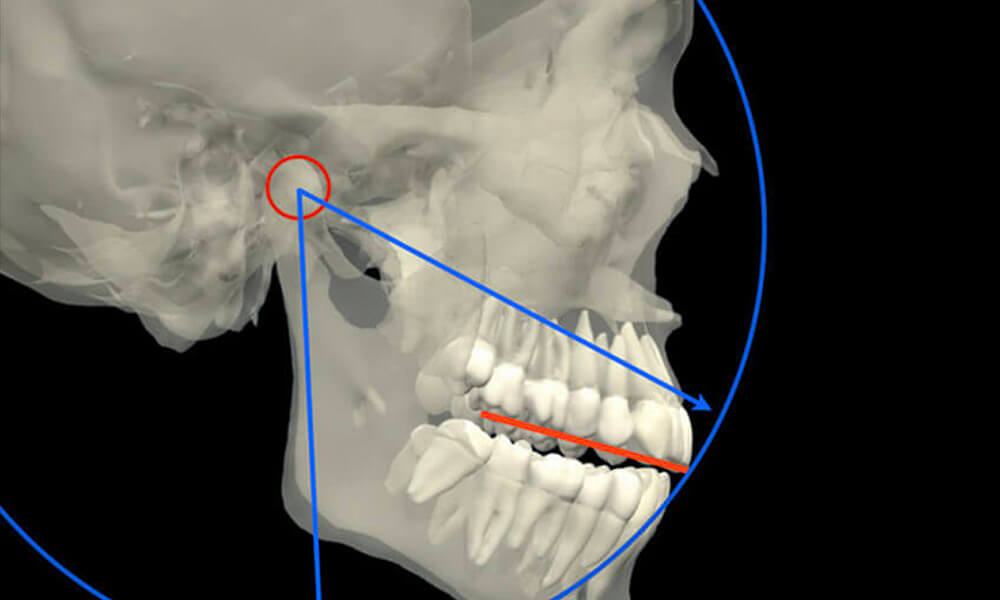
A lot of our patients have true TMD. What causes them to become symptomatic–where they have muscle issues, limited range of motion, jaw fatigue or joints trauma, myofascial pain, and they are breaking down their teeth? There are two primary causes: macro trauma and micro trauma.
- Macro trauma can cause a temporary injury to the temporomandibular system that then sets up chronic problems in the joints and muscles. This could be due to a car accident or sports incident. I have a macro-trauma patient who was hit was a lacrosse stick, another that was elbowed in the jaw during a basketball game, and a cheerleader who fell off a human tower.
- Micro trauma is what dentists call parafunction. This occurs when people put their teeth together outside the normal ways teeth touch when eating, speaking, and swallowing. We think of clenching (both static clenching and power wiggling), grinding, and tapping teeth together. We think of patients who bite their fingernails or chew on the inside of their cheeks or lips. There are lots of types of parafunctional activities. The force generated by the elevator muscles and how much of the time the muscles are overloaded leads to muscle symptoms. Accumulative force causes the excessive wear we see on teeth and damage to jaw joints.
To dentists, I say:
There are many people who have textbook malocclusions, and yet they have healthy teeth and joints. They don’t touch their teeth together outside of eating, speaking, and swallowing. There are many people with perfect occlusions who have TMD symptoms. Malocclusions don’t cause functional risk. Malocclusions don’t cause TMD. The essence of the problem is not how the teeth touch but how much they touch.
To patients with micro trauma, I say:
“You are tougher on your teeth than most of my other patients.” Staying away from psychologically negative words like clenching, grinding, and parafunction, I give them the word tougher. And I say, “You are missing more tooth structure than most people of your age.”
It is helpful for them to have this explanation before I recommend risk management strategies and pre-emptive restoration of teeth before they break.
An analogy I use with patients is the human knee. Knees don’t commonly wear out until someone is 60 to 70 years old, but long-distance runners can wear them out much earlier in life with the repetitive force of running. Our patients with parafunction put a lifetime’s worth of wear and tear on their teeth and their muscles and jaw joints in a compressed amount of time. Like a long-distance runner, their masticatory system suffers micro trauma.
It’s helpful to give patients words and analogies (like knees and car engines that wear out due to faster than normal wear and tear). I’ve had patients say to me, “I don’t like having to replace this crown, but as you said, I am tougher on my teeth than most people.”





Related Course

E3: Restorative Integration of Form & Function
DATE: October 5 2025 @ 8:00 am - October 9 2025 @ 2:30 pmLocation: The Pankey Institute
CE HOURS: 41
Dentist Tuition: $ 7400
Single Occupancy with Ensuite Private Bath (per night): $ 345
Understanding that “form follows function” is critical for knowing how to blend what looks good with what predictably functions well. E3 is the phase of your Essentials journey in which…
Learn More>
About Author
Dr. Lee Ann Brady is passionate about dentistry, her family and making a difference. She is a general dentist and owns a practice in Glendale, AZ limited to restorative dentistry. Lee’s passion for dental education began as a CE junkie herself, pursuing lots of advanced continuing education focused on Restorative and Occlusion. In 2005, she became a full time resident faculty member for The Pankey Institute, and was promoted to Clinical Director in 2006. Lee joined Spear Education as Executive VP of Education in the fall of 2008 to teach and coordinate the educational curriculum. In June of 2011, she left Spear Education, founded leeannbrady.com and joined the dental practice she now owns as an associate. Today, she teaches at dental meetings and study clubs both nationally and internationally, continues to write for dental journals and her website, sits on the editorial board of the Journal of Cosmetic Dentistry, Inside Dentistry and DentalTown Magazines and is the Director of Education for The Pankey Institute.