AI-Powered Technology in Dental Practice
Around the world, people use AI-powered technology every single day. AI algorithms generate everything from Google search results to predictive text when writing emails to speech-to-text messages on smartphones. Every time you’re shopping and see “Recommended for you,” that’s based on AI data analysis, comparing your shopping habits to those of thousands of other people.
When I spoke at the annual Pankey meeting in New Orleans in 2015, my artificial intelligence software was just in its embryotic stage. Fast forward five years, and it is on the forefront of a technological revolution that improves the operations, ROI, and patient experience in dental practices of all sizes.
Data is hindsight. Intelligence is foresight.
Artificial intelligence programs are trained by using millions of data points that were categorized by humans already. AI software is taught to recognize the meaning of what it is seeing and/or hearing. Then, AI software programs extrapolate results and apply the information to predict behavior, coach behavior, command machines, and more.
9 Ways to Leverage AI in Dental Practice
Hygiene at home: Smart toothbrushes can record how patients are brushing their teeth and share that data with dentists, typically via an app. That allows dentists to identify bad habits and teach patients how to improve their at-home hygiene routine. Some apps even remind patients when it’s time to schedule their next dental appointment.
Voice-activated commands: In healthcare, medical and dental providers are already using voice-activated technology to dictate their notes into patient electronic medical records (EMR) and to access radiographs and other images hands-free. They are also using voice commands to research symptoms, diagnostics, and treatment options. This year will see an explosion of voice-activated commands in the workplace. Gartner, Inc, a world-renowned research and advisory company, predicts 25% of digital workers will use virtual employee assistants (VEAs) daily by the end of 2021. It also predicts that by 2023, 25% of employee interactions with applications will be via voice, up from just 3% in 2019.
Pathology identification: Computer vision AI analyzes radiographs in real time to detect pathologies and standardize quality of care. It provides confidence in the dentists’ diagnostics, and ensures problems are not missed. Companies like Pearl, Videa, and Overjet are successfully implementing computer vision AI in thousands of dental practices and improving diagnosis, case acceptance and ultimately patient outcomes.
Treatment planning: AI computing models are based on the treatment plans and outcomes of hundreds of thousands of patient records. Dentists can leverage AI to analyze different treatment possibilities and determine the potential for success, the length of the case, the materials that would be used, costs, and other considerations.
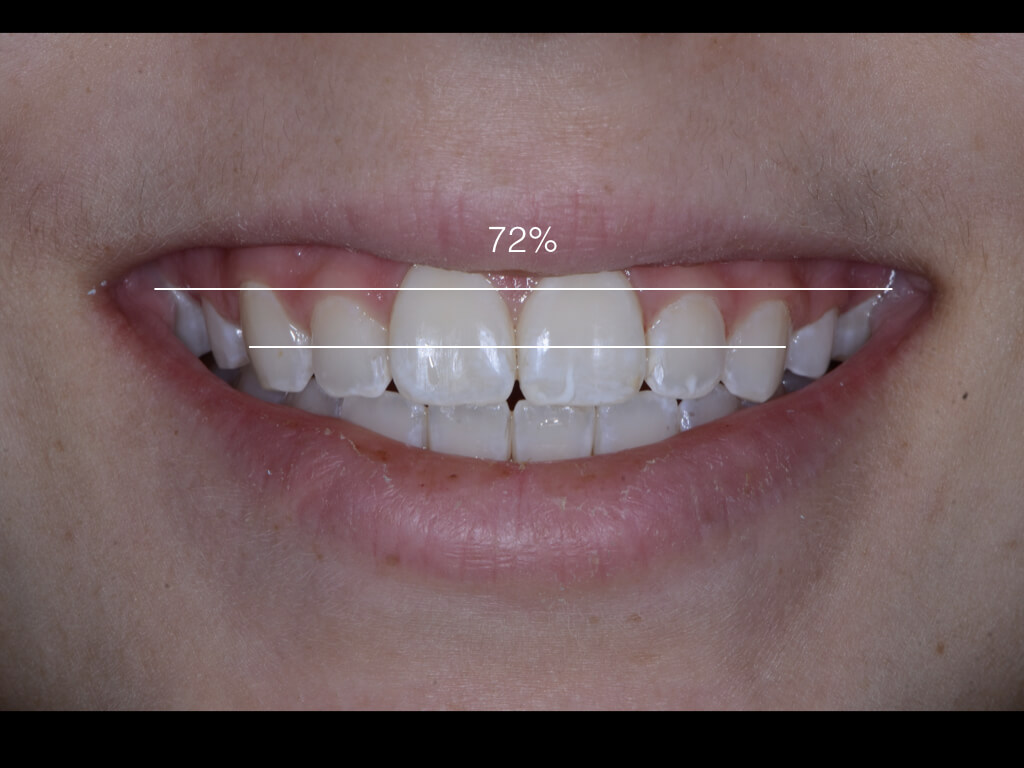
Treatment acceptance: Augmented reality isn’t just for kids’ games. Dentists use AI-powered augmented reality to generate smile designs in real time. When patients can see how the dental work will improve their appearance and restore function, they are more likely to start treatment.
Data analytics: At its most basic functionality, AI is big data computation. Its advanced algorithms predict future outcomes based on data patterns. Some dental support organizations around the country are already using AI to crunch numbers for predictive analysis designed to increase case acceptance, improve show rates, and optimize schedules.
Insurance reimbursement: For decades, insurance claims have been manually reviewed by dental professionals employed by the insurance carrier. AI can review claims, radiographs, and supporting documentation in seconds, generating approvals or identifying fraudulent claims much more quickly.
Elevated patient care: Technology has already revolutionized electronic health records. In this decade, AI will make it possible to closely tie oral health conditions to overall systemic health which will lead to better communication between providers and breakthroughs in both disease prevention and treatment.
Patient phone calls: Companies like Patient Prism leverage AI’s natural language processing algorithms and machine learning to quickly identify why patients called, the services they requested, the associated revenue, and whether the call ended in a booked appointment. Dentists use the data for everything from front office training to winning back unscheduled callers to determining whether their marketing efforts are driving the right kinds of calls.
Groups like the Artificial Intelligence Dental Council, a non-profit organization established by Pearl, are leading the way on the research and future applications. From helping patients at home to making it easier to book appointments to ensuring accuracy in diagnosis and treatment planning, AI is already revolutionizing dentistry. The future has arrived.





Related Course

E1: Aesthetic & Functional Treatment Planning
DATE: August 21 2025 @ 8:00 am - August 24 2025 @ 2:30 pmLocation: The Pankey Institute
CE HOURS: 39
Dentist Tuition: $ 6800
Single Occupancy with Ensuite Private Bath (Per Night): $ 345
Transform your experience of practicing dentistry, increase predictability, profitability and fulfillment. The Essentials Series is the Key, and Aesthetic and Functional Treatment Planning is where your journey begins. Following a system of…
Learn More>Related Article

About Author
Amol Nirgudkar is a co-founder of Patient Prism LLC and its CEO. He is a CPA, inventor, and serial entrepreneur, who speaks at dental conferences nationwide. Patient Prism holds five utility patents issued by the USPTO and is the only call tracking company that leverages artificial intelligence and human call coaching validation to analyze missed and failed new patient calls. Within 30 minutes, the AI software alerts the dental practice about lost opportunities to schedule patients seeking high value services. Call coaches prepare the Front Desk to call back that new patient with a trending success rate of 30% conversion.